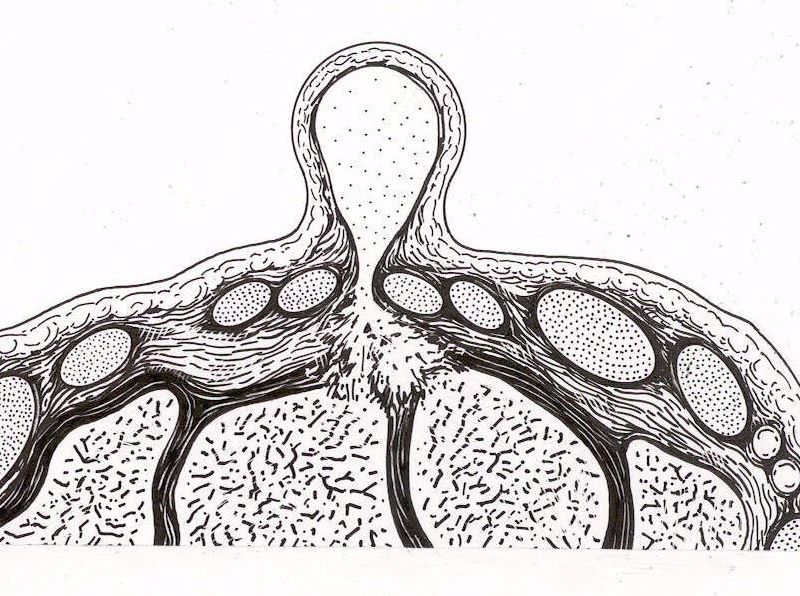
Wrist ganglia are benign tumors which are linked to an anomaly in the capsule (ligament tissue which surrounds the wrist bones). Dorsal ganglia, located on the back of the hand, are the most frequent type of synovial cysts. Palmar ganglia, located near the radial artery, are the second most frequent. Fairly often, degenerative microcysts appear near the initial ones.
There are no known predisposing factors.
Most often, the cause for the occurence of a ganglion is unknown. However, in some cases, it is possible to observe a post-traumatic onset of synovial cysts. In such cases, one should check for associated ligament lesions.
The evolution of ganglia, whether dorsal or palmar, is very particular. Very often, they appear during a specific period and then tend to completely disappear. They are seldom painful. However, in some cases, the excess in internal pressure may lead to pain. Occasionally, their disappearance may take several months. When they remain, depending on their size, the discomfort they generate may be only esthetic or, at times, functional by limiting the wrist range of motion and decreasing the muscle strength.
Simple AP and lateral view X-rays of the wrist bones can help determine whether there any traumatic lesions related to the cyst (such as fractures, scapholunate dissociation, arthritis…). When the actual localization of the cyst is unclear, the physician can request an MRI (Magnetic Resonance Imaging). This completely harmless medical exam explores soft tissue and will help determine the exact cause of the cyst.
A number of treatment methods have been put forward, from abstention to open surgery.
Medical TreatmentMost often, ganglia are benign tumors without consequences (except cases where the cyst is related to a traumatic lesion). As such, patients generally wish to remove them for cosmetic reasons. Then a medical treatment may be indicated.
The treatment may involve a simple injection or percutaneous needle evacuation of the ganglion, knowing that recurrence is almost certain in a majority of cases. The method consisting in crushing the cyst with a coin, as put forth by some of our former colleagues, is both painful and ineffective.
Surgical TreatmentThere are two types of surgical treatment:
- “Open” surgical treatment, which consists in a normal procedure during which the surgeon incises the skin, then dissects the ganglion down to its origin and removes it with part of the joint capsule which is responsible for the cyst. Dorsal ganglia are less risky to operate on than palmar ganglia, as the latter are located near the radial artery.
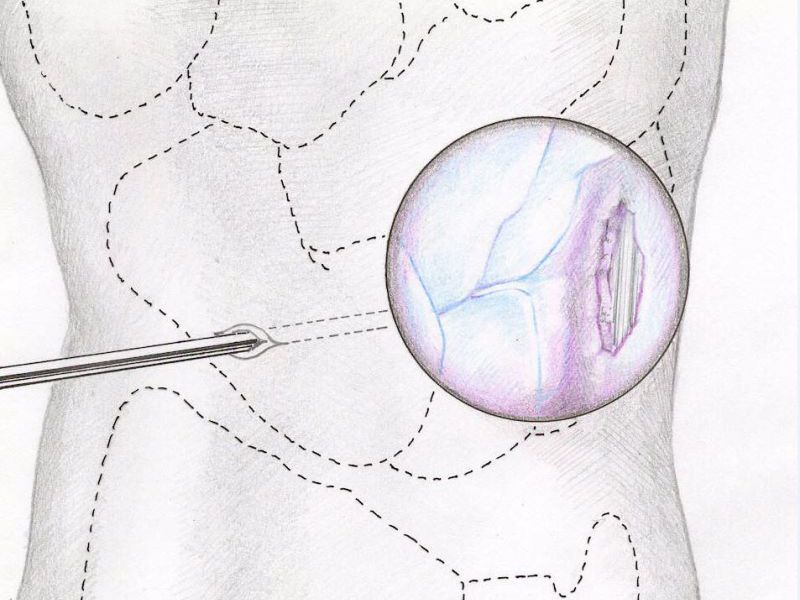
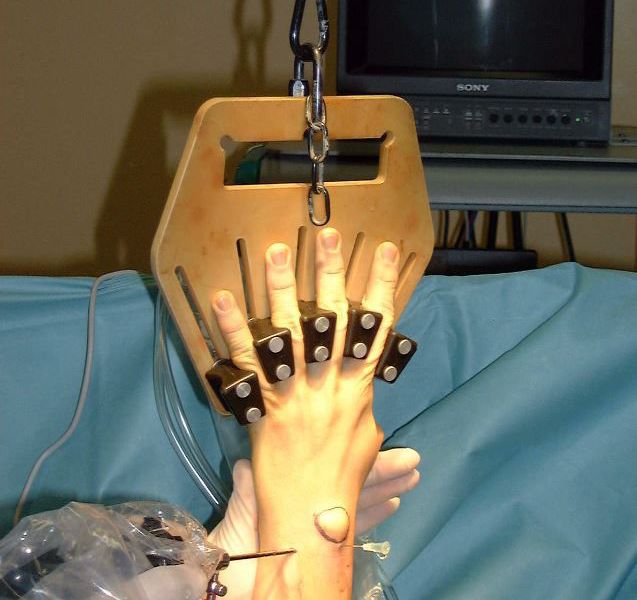
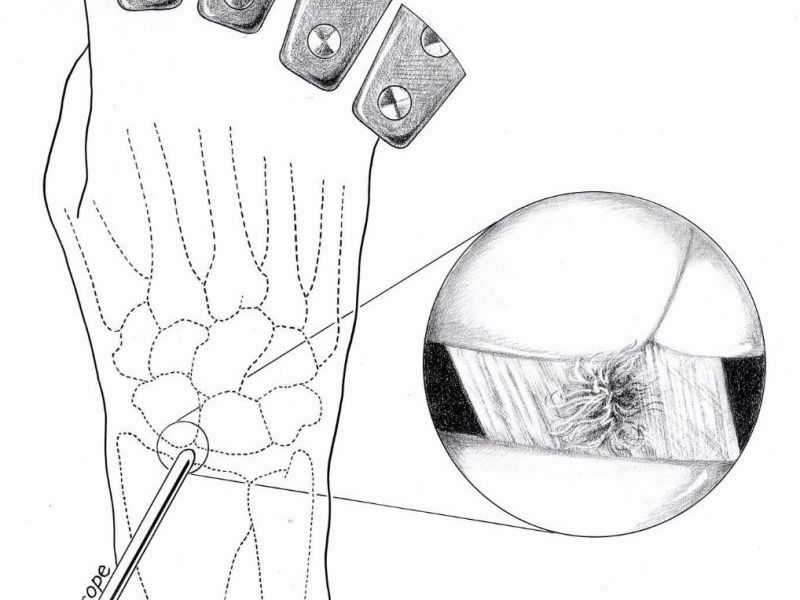
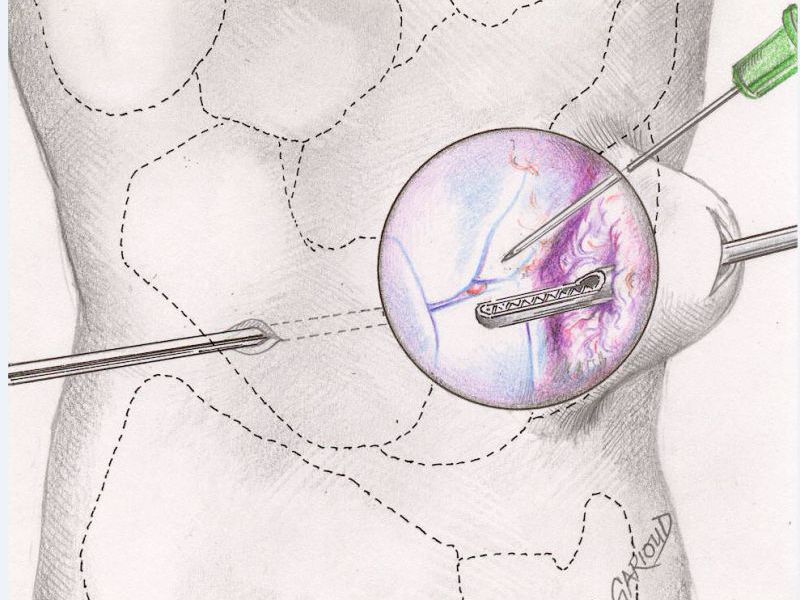
- Arthroscopic treatment, which is a simpler technique for the patients. Through two small openings the size of which does not exceed 2 millimeters, and do not require stitches, the surgeon uses a camera to look inside the wrist join and find the cyst’s origin. Thanks to miniature instruments, the surgeon may then remove the cyst’s origin, the adjacent capsule, and the cyst wall. Patients can use their hands immediately after surgery. There are no stitches which need to be removed. This technique can also be performed for anterior ganglia as the cyst removal process takes place away from the radial artery, therefore decreasing the risk of damaging it.
With open surgery techniques, there are two classical complications : unsightly scars, and mobility loss (especially for dorsal ganglia). In the case of palmar ganglia, the proximity of the radial artery might cause lesions of the latter, which will in turn require surgical repair during the same procedure.
There are very few complications for arthroscopic surgery, since such procedures leave no cosmetic sequelae and produce no loss of mobility.
For both techniques, the most common complication is recurrence of the cyst, which is unforeseeable. Regardless of the surgical technique, recurrence happens in 10% of cases. In case of recurrence, both surgical techniques may be used, regardless of which technique was originally employed.
A comfortable dressing is put in place for a few days. For dorsal cyst removals, some physicians recommend a splint for 2 weeks. Scar management is minimal after open surgery and nonexistent after arthroscopy.
Finger movement is possible immediately after surgery. In the case of arthroscopy, hand and wrist motion is possible immediately in the postoperative period.
After the procedure, simple analgesic and anti-inflammatory drugs may be prescribed to treat initial pain, which is usually minimal anyways.
The leave of absence will depend on the patient’s occupation. In some cases it isn’t necessary, and in others it may last 2 weeks or up to a month.
How fast patients will recover the use of their hand and their muscle strength depends on which surgical technique was used and on their own sensitivity. Most often, complete use of the hand is possible after 3 weeks, even for sports activities requiring forceful use of the hand.





In 20 years of existence, the INSTITUT DE LA MAIN has become one of the main hand and upper limb surgery centers in Europe. Its nine surgeons on staff can treat all hand and upper limb problems.
Institut de la Main
Clinique Bizet
21 rue Georges Bizet
75016 PARIS
Front Desk : +331 84 13 04 56
Hand Emergencies : +331 84 131 131




